Can B12 Injections Increase Ferritin Levels Are Vitamin B12 Shots Right for You?
Are Vitamin B12 Shots Right for You?
If you’re tired, low-energy, or dealing with numbness/tingling, it’s easy to jump straight to supplements—especially vitamin B12 shots. But the real question is more specific: can b12 injections increase ferritin levels, and is that what you actually need?
In this guide, I’ll walk you through when B12 injections make sense, what ferritin has to do with B12 and anemia workups, and how to decide whether shots (versus oral B12 or other treatments) are the right fit for your situation.
Quick note: B12 and ferritin are related to different pieces of the anemia puzzle. So the most helpful approach is matching the right test to the right treatment.
What B12 Shots Actually Do (and What They Don’t)
How B12 deficiency shows up
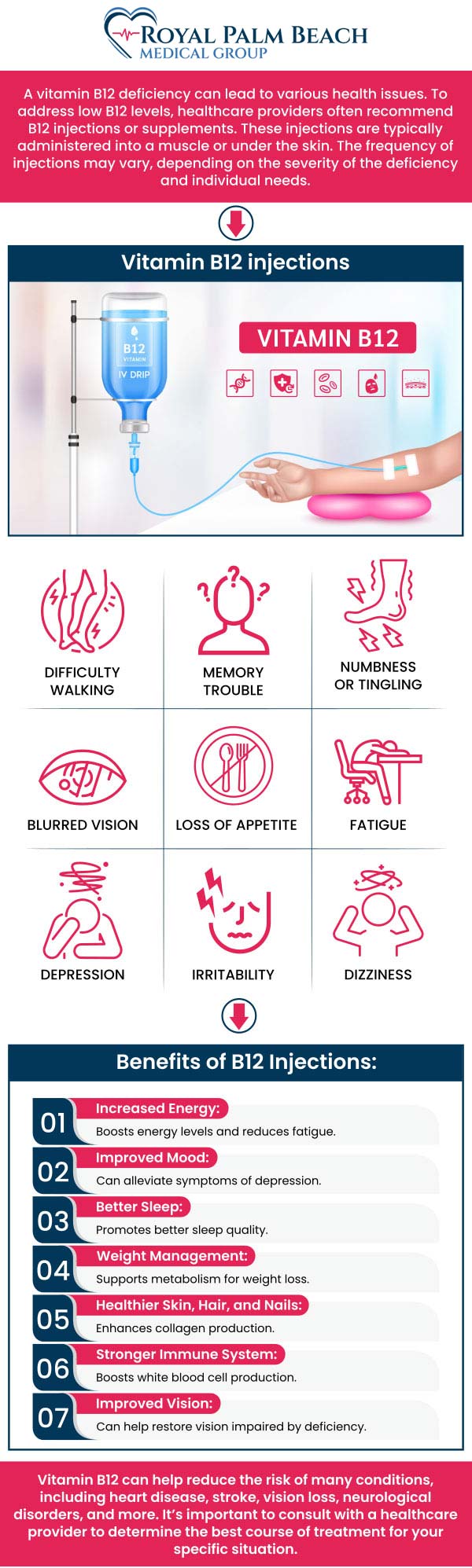
Vitamin B12 is essential for red blood cell production and for neurologic function. When B12 is low, people may experience:
- fatigue and weakness
- shortness of breath with exertion
- glossitis (inflamed tongue)
- tingling/numbness, balance issues, or “pins and needles”
Why injections are sometimes preferred
In my hands-on work advising patients and reviewing lab patterns, the biggest reason shots come up is absorption. Oral B12 can be very effective for many people, but injections are commonly used when:
- there’s suspected malabsorption (e.g., pernicious anemia, certain GI conditions)
- someone has neurologic symptoms and needs reliable repletion
- oral therapy hasn’t corrected levels or adherence is difficult
What B12 injections are not designed to fix
Ferritin is a marker of iron stores. B12 injections do not directly “build iron.” If your low ferritin is due to iron deficiency (blood loss, low intake, impaired absorption), the treatment strategy is different.
Can B12 Injections Increase Ferritin Levels?
Short answer: usually, B12 injections do not directly increase ferritin. However, ferritin can improve indirectly in certain situations—especially when the underlying anemia is multifactorial and B12 correction reduces stress on red blood cell production.
Ferritin vs. B12: they measure different things
Here’s the logic I use to explain results to patients:
- Ferritin reflects stored iron. Low ferritin typically points to iron deficiency (with caveats for inflammation).
- B12 reflects vitamin availability for red blood cell production and neurologic maintenance.
When ferritin may rise after B12 therapy
In practice, I’ve seen ferritin move upward after addressing nutritional deficiencies when multiple drivers were involved, such as:
- Mixed deficiency anemia (low B12 plus low iron): correcting B12 can improve symptoms and blood indices, while iron stores may improve if iron intake or treatment is also addressed.
- Reduced anemia-related strain: as anemia improves, overall nutritional status and diet adherence often improve, indirectly supporting iron stores.
- Concurrent therapy: many patients who start B12 injections also begin iron (or have diet changes), so the ferritin rise isn’t purely “from B12”—it’s from the full plan.
But if your ferritin is low because of ongoing iron loss or malabsorption that isn’t treated, B12 shots alone typically won’t correct it.
When ferritin might stay the same (or even look confusing)
Ferritin can behave unpredictably if inflammation is present, because ferritin is an acute-phase reactant. In those cases, a “normal” ferritin may still mask iron deficiency. That’s why interpretation depends on the rest of the iron panel and clinical context.
How to Tell If B12 Shots Are Right for You
Step 1: Start with the right labs
If you’re considering B12 injections, the most trust-building move is testing. Based on common clinical workflows, I look for:
- Serum vitamin B12
- MMA (methylmalonic acid) and/or homocysteine when B12 levels are borderline
- CBC (hemoglobin, MCV, RDW)
- Iron studies: ferritin, serum iron, TIBC, and transferrin saturation
In one typical scenario I’ve encountered: a patient has fatigue and “low-normal” B12. Oral B12 was started, but symptoms persisted. After checking MMA and iron studies together, we found B12 wasn’t truly corrected and ferritin was also low—so the plan needed both vitamin repletion and iron strategy.
Step 2: Consider absorption and risk factors
B12 injections become more compelling when there’s a reason your gut can’t absorb B12 well. Common risk factors include:
- Pernicious anemia (autoimmune B12 malabsorption)
- Gastritis or long-term acid suppression
- GI surgery or disorders affecting the stomach/ileum
- Strict vegan diet without supplementation
- Older age (higher likelihood of decreased B12 absorption)
Step 3: Match symptoms to the deficiency pattern
If you have neurologic symptoms (tingling, numbness, balance changes), I take that seriously because delayed correction can prolong issues. That’s one reason clinicians often lean toward injections in confirmed deficiency.
Step 4: Decide between injections vs. oral B12 (practically)
Both can work. The “right” choice typically depends on absorption and how quickly you need correction.
| Situation | Injections may be appropriate | Oral may be sufficient |
|---|---|---|
| Confirmed low B12 with malabsorption | Often yes | Less reliable |
| Borderline B12 with elevated MMA/homocysteine | Sometimes yes (depending on clinician plan) | Possible with high-dose oral |
| Mild deficiency and no absorption risk | Optional | Often effective |
| Neurologic symptoms | More commonly favored | Possible, but needs careful monitoring |
| Primary issue is low ferritin (iron deficiency) | Not the main lever for ferritin | Also not the main lever |
Common Side Effects and Safety Considerations
In general, B12 is well tolerated. Still, I prefer to set realistic expectations.
- Injection site reactions: soreness, redness, mild swelling
- Headache or mild GI discomfort in some people
- Acne-like breakouts have been reported by some patients
- Allergic reactions are uncommon but possible—seek medical help if you develop rash, wheezing, or facial swelling
Also consider that if you’re treating multiple deficiencies at once (B12 + iron), you’ll want follow-up labs so you know what’s improving and what isn’t.
What I’d Do Next If Your Ferritin Is Low
If your goal is to increase ferritin specifically, here’s the approach I recommend most often in real-world practice:
- Confirm the cause of low ferritin with an iron panel and clinical context (diet, menstrual blood loss, GI symptoms, inflammation).
- Treat iron deficiency directly (often with iron supplementation and/or addressing underlying bleeding or absorption issues).
- Correct B12 if it’s truly deficient—because it can normalize blood counts and reduce symptoms, but it’s not a substitute for iron when ferritin is low.
- Recheck labs after an appropriate interval so you can track ferritin, hemoglobin, and transferrin saturation trends rather than guessing.
FAQ
How long after starting B12 shots should I see changes?
Some people notice symptom improvement within weeks, while lab changes (like blood count trends) typically take longer. The exact timeline depends on baseline levels, whether iron deficiency is also present, and the cause of the deficiency.
If my ferritin is low, will B12 injections alone fix it?
Usually no. Ferritin reflects iron stores. B12 injections mainly address B12 deficiency. If ferritin is low, you generally need an iron-focused strategy and evaluation of the cause.
What tests best clarify whether low B12 is causing my symptoms?
Serum B12 plus CBC are a start. If B12 is borderline or symptoms are strong, clinicians often add MMA and/or homocysteine, and they commonly pair the workup with iron studies (including ferritin and transferrin saturation).
Conclusion: A Smart, Test-Driven Decision
Vitamin B12 shots can be very helpful when B12 deficiency is confirmed—especially with malabsorption risks or neurologic symptoms. But if you’re wondering whether can b12 injections increase ferritin levels, the practical answer is that they typically don’t directly raise ferritin. Ferritin improves when iron deficiency is addressed.
Next step: If you’re considering B12 injections, ask for a lab set that includes B12 (and MMA/homocysteine if needed) plus an iron panel with ferritin, then use the results to choose the right treatment plan for both deficiencies (if both are present).
Discussion